






My goal here is not to influence your life decisions but to open your eyes to research and information that you won’t find in Forbes or other business and investment publications.
After reading this, perhaps you will not only gain a new perspective but, more importantly, learn how real research can give you access to insights not found in today’s mainstream media.
In fact, I will provide a direct source for every point I make – as much of what you’re about to read is highly controversial to what the government and media are telling you.
Once you understand this, perhaps you can use it to influence all of your future decisions – be it investing or life decisions.
Read this with an open mind.
Due Diligence
The most successful investors spend the majority of their time on research. We call this due diligence.
And the best of the best investors, those who win time and time again, almost always do more due diligence than others.
This due diligence is what separates the average investor (the retail investor) from a highly successful one (the pros).
The average retail investor might have read a tweet or a Facebook post telling them that shares of XYZ are about to go higher. A better retail investor might have read an N.Y. Times article that told them XYZ was a bargain. And a more seasoned retail investor might even go to XYZ’s website and look through news releases and presentations.
But that’s the problem.
Should you trust a tweet from some random person? Should you trust an N.Y. Times article written by a journalist who never invested in his life? Should you rely only on a company’s presentation on their website, knowing that the primary role of presentation are to attract and maintain investors?
The answer to all of those questions is a hard no. Yet, that is how the majority of retail investors conduct due diligence.
This is the basic psychology of the masses.
It’s why the banks and funds win and retail investors lose.
It’s also why our world is where it is today: divided.
Mass Psychology is Real
Politicians and the elite understand the theory of mass psychology extremely well. They use it to their advantage to maintain control of the masses. When empires reach a peak, rulers of those empires often pit citizens against one another, so the citizens turn on each other rather than the rulers.
We’re witnessing this now.
First, it was political: Left vs. Right.
Then it became racism: everyone against whites.
And now, it has become pro-covid vaxxers vs. anti-covid vaxxers.
Instead of looking from another’s perspective, most people have become extremely intolerant. Perhaps the pandemic caused this. Perhaps the media did. Perhaps the politicians who created the lockdowns did.
No matter the true reasons, let’s remain human and understand that there is always more than one point of view, especially regarding our livelihoods.
Locking citizens in their homes for months upon months, killing businesses, rolling out vaccines with less than one year of observation to billions of people, and still, we’re not even close to being out of this so-called pandemic.
So whatever your biases, let’s take a step back today and look at things from a professional investor’s point of view.
When the Pros look to invest, they’ll look through public documents, filings, presentations, third-party research, analyst reports, market forecasts, and even conduct interviews with anyone close to the company. Heck, they sometimes even call that company’s clients and competitors.
Not one pro I know relies on headlines and news articles – and especially not fact-checkers.
While professional investors always begin their due diligence at why they should invest in a company, much more time is spent on why they shouldn’t. In other words, they question everything before making an investment decision.
So when it comes to the debate between those for and against the Covid-19 vaccines, especially one that has ZERO long-term studies, why are the majority of people acting like retail investors?
Because, just like investing, that is the basic psychology of the masses.
“The masses have never thirsted after truth. They turn aside from evidence that is not to their taste, preferring to deify error, if error seduce them. Whoever can supply them with illusions is easily their master; whoever attempts to destroy their illusions is always their victim.”
-Gustave Le Bon-
I’ll give you one example.
The Fate of Billions
Pfizer is a public company. That means they have filings and news releases that anyone can dig through when researching Pfizer’s COVID-19 vaccine.
But how many of you looked through them? Be honest.
Share your honesty by clicking here.
Pfizer’s Phase 3 trial was actually quite robust in that it had 43,661 participants. Half received the vaccine; half placebo.
To determine effectiveness, Pfizer monitored how many people came back after their shots and tested positive for COVID-19. For example, if 10 participants were tested positive for COVID-19 following their injections, and only one of those participants had the vaccine, they would say the effective rate of the vaccine is 90%.
So, of the more than 43,000 trial participants, how many do you think had to come back and test positive for COVID-19 to conclude the trial and prove efficacy rate?
If you didn’t know this, hold on to your hats.
170.
That’s a mere 0.389% of the entire study group.
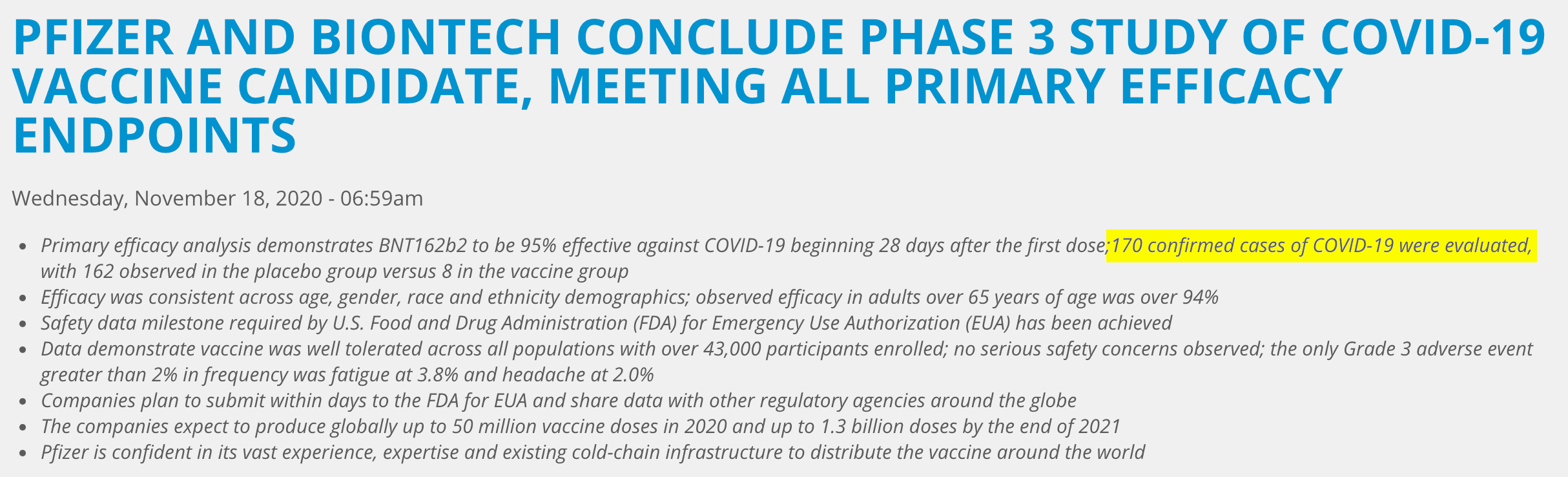
Here’s the source: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine
That’s what paved the way for Pfizer to do this:
Via Pfizer:
“Based on current projections, the companies expect to produce globally up to 50 million vaccine doses in 2020 and up to 1.3 billion doses by the end of 2021.”
Be honest, did you know that?
Click here to comment
Pfizer’s not alone here. All of the emergency COVID-19 vaccine creators had similar phase 3 trials.
So, instead of being angry at each other for having different views, let’s act like professional investors and question everything today.
I’ll lay out the facts and source everything, so you don’t have to.
If support the COVID-19 vaccines, this might change your mind; if you’re against it, this might change your mind.
Either way, you’ll be armed with more ammo to debate. And if you’re an investor, hopefully, you’ll do more of your own due diligence moving forward.
The Numbers
Just like looking at a company’s financial statements, let’s look at the numbers for the COVID-19 vaccines – as we did with the Pfizer example above.
The COVID-19 vaccines are part of the biggest and fastest vaccination campaign in history. As of today, more than 360 million doses have been administered in the U.S. alone, and more than 4.85 billion doses have been administered globally.
Here is the source: https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/
Since millions of people around the world aren’t dropping dead as a result, many will argue that the vaccines are mostly safe.
But how safe? Let’s look at the numbers…
In the U.S., the CDC has a system to track (as best as they can) adverse vaccine reactions. This system is called the Vaccine Adverse Event Reporting System, better known as VAERS.
You can find the system here: https://wonder.cdc.gov/vaers.html
According to this system, and as of August 6th, 2021, searching the system for COVID-19 vaccines shows that it has recorded 12,791 deaths, 16,044 permanent disabilities, 70,667 emergency room visits, 51,242 hospitalizations, 13,139 life-threatening events, with 682,873 reported injuries of which 571,831 cases had an association with a COVID-19 vaccine. The 12,791 deaths do not include the 1360 fetal deaths following a COVID-19 vaccine, which can be found by using the appropriate endpoints in VAERS.
To be fair, let’s keep this in context:
- VAERS accepts reports of any adverse event following any vaccination.
- Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem, i.e., fetal deaths could have been from abortion due to many reasons.
The CDC has also stated that these statistics may or may not be related to the COVID-19 shots. Source: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
Now, 12,791 deaths don’t seem like a lot compared to the millions who have received a shot in America. But tell that to one of the families who might have lost a loved one to the vaccine*.
(*The media has interviewed hundreds of people who have lost a loved one due to COVID, but not one who has lost someone due to the vaccine. The greater good, right?)
But let’s continue keeping things in context – after all, we’re only talking numbers here.
How do the COVID-19 vaccines stack up to other vaccines?
According to VAERS, all FDA-approved vaccines over the last 30 years have been linked to just 6,068 deaths.
In other words, there have been twice as many deaths over the last nine months following a COVID-19 vaccination than ALL FDA-approved vaccines over the past 30 years combined. Source: https://wonder.cdc.gov/vaers.html
Now, one could argue that this results from the largest vaccination campaign in history, hence the much bigger numbers. But, conversely, one could argue that if you tallied all of the vaccines administered to Americans last year, including flu and all others, it would total more than 300 million doses – very similar to the amount of COVID shots administered thus far.
That’s also just in the U.S. – there have been over 4.86 billion doses administered worldwide.
If you include the reporting systems from EudraVigilance (E.U., EEA, Switzerland), and MHRA (U.K.), these systems have now recorded more Injuries and Deaths associated with COVID-19 vaccines than from all previous vaccines combined since records began.
Source: https://www.ema.europa.eu/en/human-regulatory/research-development/pharmacovigilance/eudravigilance
Source: https://www.gov.uk/government/organisations/medicines-and-healthcare-products-regulatory-agency
As of August 1st, 2021, over 34,000 Covid-19-linked deaths and over 5.46 million injuries were reported via VAERS, EudraVigilance, MHRA.
One could further argue that only a fraction of the adverse reactions is actually ever reported.
For example, according to a former New York Times reporter, Alex Berenson, on August 6th:
“Covid vaccine maker Moderna received 300,000 reports of side effects after vaccinations over a three-month period following the launch of its shot, according to an internal report from a company that helps Moderna manage the reports…That figure is far higher than the number of side effect reports about Moderna’s vaccine publicly available in the federal system that tracks such adverse events.
The 300,000 figure comes from an internal update provided to employees by IQVIA, a little-known but enormous company that helps drugmakers manage clinical trials. Headquartered in North Carolina, IQVIA has 74,000 employees worldwide and had $11 billion in sales last year.”
“Earlier this week, Richard Staub, the president of IQVIA’s Research & Development Solutions division, sent a ‘Q2 2021 update’ which was labeled ‘Confidential – For internal distribution only.”
“A person with access to the presentation provided screenshots of the relevant slide, which clearly explains the 300,000 side effect reports were received over ‘a three-month span’ – not since the introduction of the vaccine in December…”
Source: https://alexberenson.substack.com/p/some-actual-news
Now, to be fair, I haven’t been able to confirm with IQVIA to determine if this update exists – and given the confidential nature of the partnership between IQVIA and Moderna, I likely never will.
But ask yourself:
“Is every death in the U.S. being cross-referenced to someone who had a COVID vaccine?”
“Is everyone who has some sort of reaction reporting it to VAERS?”
A 2010 Harvard Pilgrim Health Care, Inc. study of VAERS’ reporting numbers showed that fewer than 1% of vaccine adverse events are ever reported.
Via the study:
“Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA).
Likewise, fewer than 1% of vaccine adverse events are reported.”
If those numbers remain true today, then one could argue that the number of adverse events from the COVID-19 vaccines could be over 57 million (571,831 injuries reported times 100*) in the U.S., and over half a billion globally (5.4 million injuries reported times 100*).
(*based on the study that shows fewer than 1% of vaccine adverse events are reported.)
Of course, one could also argue that VAERS has improved over the last ten years, and not every adverse reaction reported directly resulted from the COVID-19 vaccine. One could also argue that many adverse reactions from other vaccines were underreported as well.
As you can see, the problem with data and numbers is that both can easily be manipulated to suit a particular narrative.
For example, I could use the above data and overzealously extrapolate overhyped anti-COVID-vaccine headlines such as:
“Data shows COVID-19 vaccines have potentially injured half a billion people,”
“Data shows COVID-19 vaccines have potentially killed over 3.4 million, due to underreporting.”
*(34,000 deaths times 100)
See what I am saying?
Yet, this is precisely what has happened and continues to happen today.
Let’s start with the chain of events.
The Test
In order for a pandemic to be a pandemic, it has to affect a lot of people.
So there must be a test that determines if someone is sick or infected. For COVID-19, the gold standard test is the RT-PCR test.
I explained what this test is back in November 2020. You can find it here: https://www.equedia.com/everything-you-need-to-know-about-covid-rt-pcr-testing-and-the-boldest-prediction-of-2020/
In that letter, I also explain how test labs were using a C.T. value of 40 or higher when determining COVID-19 cases, which was absurd because anything over 35 was useless.
Via NYT:
“Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think that 40 could represent a positive,” she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on.”
Can you see the problem here? Could it be that the millions of positive COVID cases reported were reported incorrectly simply by the misuse of data?
What would happen if we used a lower Ct?
It turns out, the NYTimes also wanted to know. And they found out last year.
Via NYT, continued:
“In three sets of testing data that include cycle thresholds (Ct), compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found.
On Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times.
If the rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually need to isolate and submit to contact tracing.”
In other words, the data suggests that only 10% of those who tested positive for COVID may actually be infectious and need to isolate, if they’re even sick or contagious at all.
That was then. So, where are we now when it comes to these tests?
It turns out, according to a consortium of scientists with great knowledge of this, 10% is an understatement.
Via Cormandrosten Review:
“…if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the U.S.), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97%.”
Feel free to look up the credentials of all the experts within that report. I did.
Even the World Health Organization (WHO) indirectly admitted that using a high Ct value creates too many false positives and that every test that used a high Ct should be retested.
Via WHO:
“Careful interpretation of weak positive NAAT results is needed, as some of the assays have shown to produce false signals at high Ct values. When test results turn out to be invalid or questionable, the patient should be resampled and retested.”
Despite all of this, the majority of tests used around the world still use Ct values greater than 35.
But why?
I am not entirely sure. But would people continue to support the vaccines if cases continue to drop? What do you think?
Click here to share your opinion
The Vaccine Conundrum
We already know that many top-level doctors have used Ivermectin on themselves and colleagues with great effect. For example, last year, I watched a live video of a top U.S. doctor telling Congress that he and multiple nurses have used Ivermectin and that not one of them caught COVID-19.
That video has since been taken down, despite it being a live U.S. government hearing. The question is, why?
One can only assume that if such a treatment existed, then an emergency vaccine would never have been approved – since that is the legal framework behind Emergency Use Authorizations.
Now, I am not saying Ivermectin is better than any of these vaccines or if it even works. And I am certainly not saying I am recommending it – but don’t you want to know why it’s quietly being touted by some of the top doctors around the world?
Let me share with you just one paper on this.
From June 2020, via Science Direct:
“Ivermectin is an inhibitor of the COVID-19 causative virus (SARS-CoV-2) in vitro.
A single treatment able to effect ~5000-fold reduction in virus at 48 h in cell culture.
Ivermectin is FDA-approved for parasitic infections, and therefore has a potential for repurposing.
Ivermectin is widely available, due to its inclusion on the WHO model list of essential medicines.”
That’s right. Ivermectin is deadly against COVID-19…in vitro. But there’s more.
Via Monash University:
“A collaborative study led by the Monash Biomedicine Discovery Institute (BDI) with the Peter Doherty Institute of Infection and Immunity (Doherty Institute), a joint venture of the University of Melbourne and Royal Melbourne Hospital, has shown that an anti-parasitic drug already available around the world kills the virus within 48 hours.
The Monash Biomedicine Discovery Institute’s Dr. Kylie Wagstaff, who led the study, said the scientists showed that the drug, Ivermectin, stopped the SARS-CoV-2 virus growing in cell culture within 48 hours.
“We found that even a single dose could essentially remove all viral RNA by 48 hours and that even at 24 hours there was a really significant reduction in it,” Dr. Wagstaff said.
…Although the mechanism by which Ivermectin works on the virus is not known, it is likely, based on its action in other viruses, that it works to stop the virus ‘dampening down’ the host cells’ ability to clear it, Dr. Wagstaff said.
Royal Melbourne Hospital’s Dr. Leon Caly, a Senior Medical Scientist at the Victorian Infectious Diseases Reference Laboratory (VIDRL) at the Doherty Institute where the experiments with live coronavirus were conducted, is the study’s first author.
“As the virologist who was part of the team who were first to isolate and share SARS-COV2 outside of China in January 2020, I am excited about the prospect of Ivermectin being used as a potential drug against COVID-19,” Dr. Caly said.”
So why hasn’t this been pursued further? Why hasn’t the government provided more funding for this – especially considering billions have been poured into vaccines?
Don’t you want to know? I’ve reached out to Monash University, and I am awaiting a response. I will update everyone here if I receive a comment back.
The Vaccine Works…or Does it?
With millions around the world having received their jabs, there is no turning back for the governments who continue to push the mRNA covid vaccines – recall that AstraZeneca, the more traditional vaccine, is not recognized in the U.S.
If the mRNA vaccines turn out to be ineffective or not as effective as once thought, you can surely bet the citizens of the world will revolt. So, you can understand why there is such a rush for segregating those who are vaccinated and those who aren’t.
Yet, despite the majority of the N. American population being fully vaccinated, cases are once again climbing back up. But why?
Well, let’s start by blaming those who are unvaccinated.
The Unvaccinated
On July 16th, 2021, CDC director Dr. Rochelle Walensky said that “over 97% of people who are entering the hospital right now are unvaccinated.”
She went so far as to say: “There is a clear message that is coming through: This is becoming a pandemic of the unvaccinated.”
That’s pretty crazy messaging – one that was obviously designed to segregate the vaccinated and the unvaccinated.
But remember, data and numbers can easily be skewed to sway an opinion.
It didn’t take long before someone called Dr. Walensky out on her misuse of the data.
Here’s the video:
https://video.foxnews.com/v/video-embed.html?video_id=6266738894001&
It turns out the data Walensky used when she said “97% of those entering the hospital right now were the unvaccinated” wasn’t actually from “right now.” It was data gathered by the CDC between January through June 2021.
In fact, Walensky’s “right now” didn’t even include any recent data.
Why is that grossly misleading?
Well, on January 1st, 2021, only 0.5% of the U.S. population had received their jab. It wasn’t until mid-April that an estimated 31% had received one or more shots.
So, since most people weren’t fully vaccinated during that period, it would be quite obvious that those experiencing severe covid-19 symptoms would be the unvaccinated.
Canada has been no different in its reporting.
Take a look:
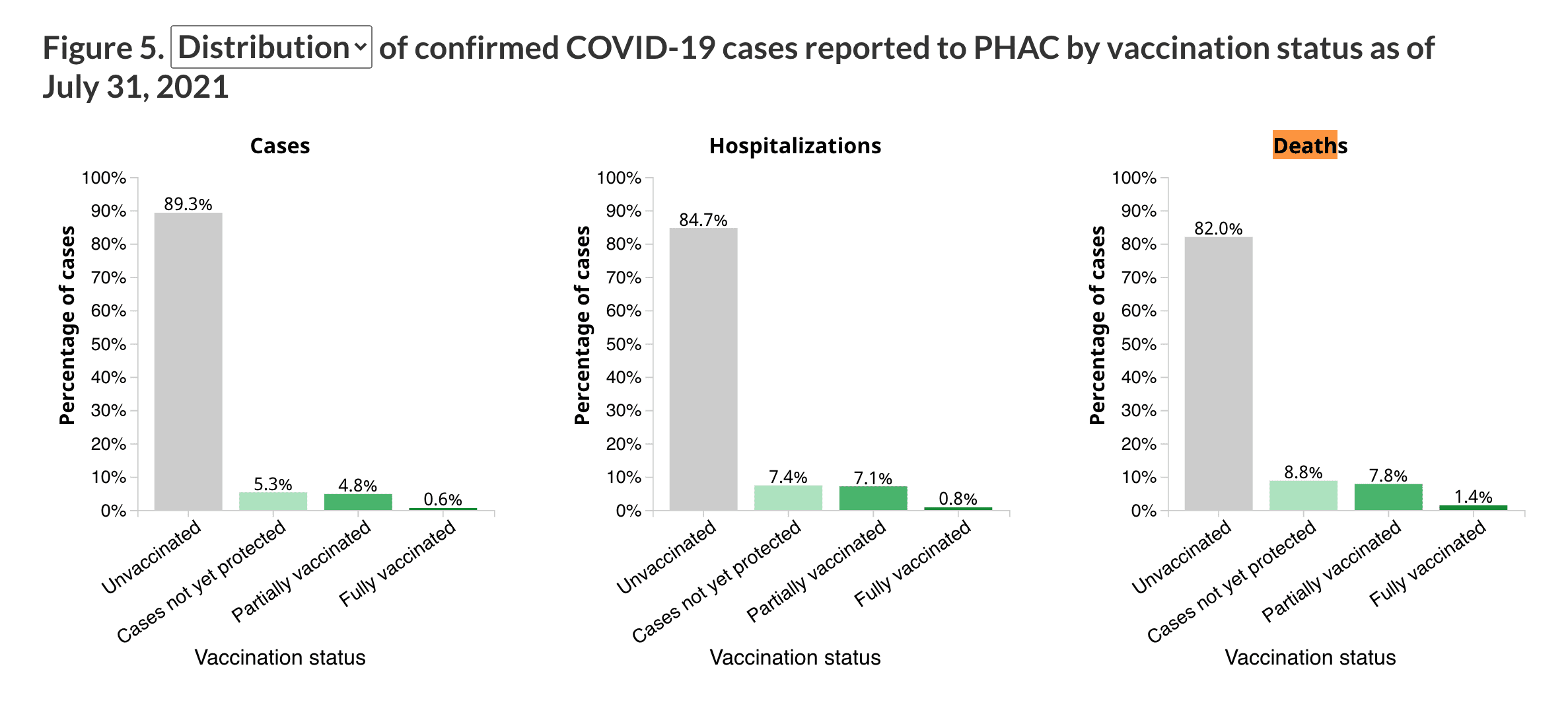
Here, again, the data is extracted on August 16th, 2021, for cases from December 14th, 2020, up until July 31st, 2021.
Take a look at this:
https://health-infobase.canada.ca/covid-19/epidemiological-summary-covid-19-cases.html
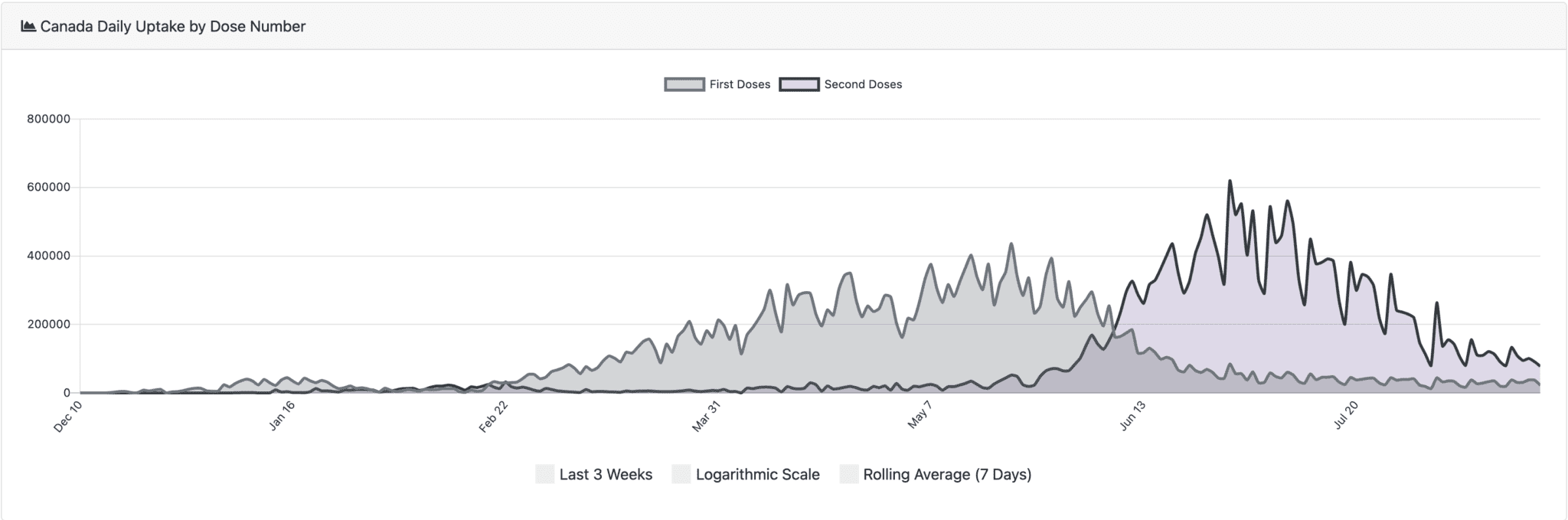
It doesn’t take a mathematician to see that fully vaccinated individuals didn’t reach any significant numbers until mid-late June.
And most of the cases occurred prior to anyone being fully vaccinated.
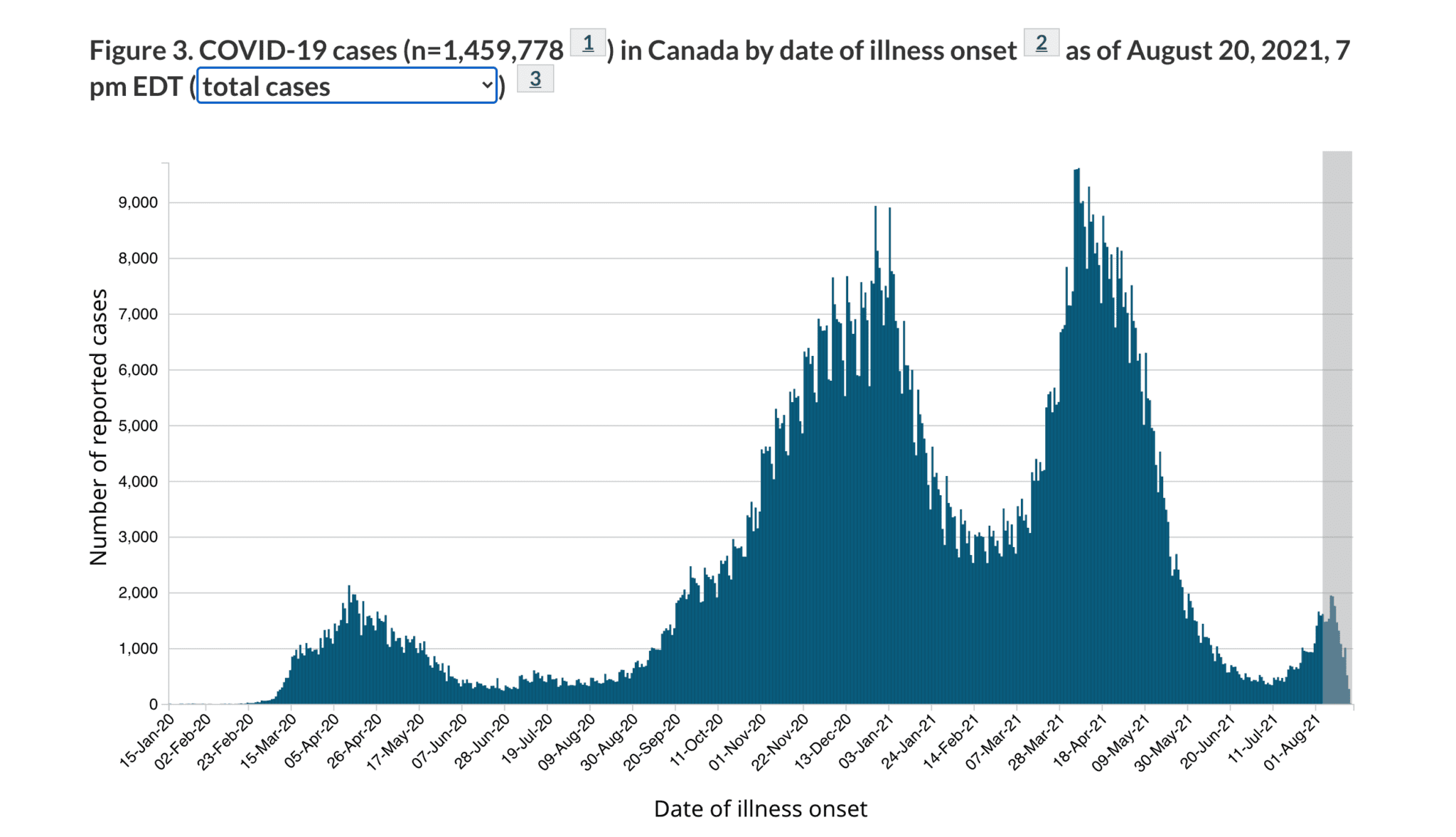
If you further look at deaths, the majority occurred in January 2021 – before the vaccine rollout.
Sure, one could argue that deaths and cases have dropped as soon as the vaccine campaign began earlier this year.
But one could also argue that it could be the result of the weather.
As I mentioned in March 2020:
“…the virus responsible for COVID-19 is wrapped in an envelope of fat. In warmer climates, the heat gets rid of the fat layers of the virus much faster. Without that fat, the virus can’t survive.”
Take a look:
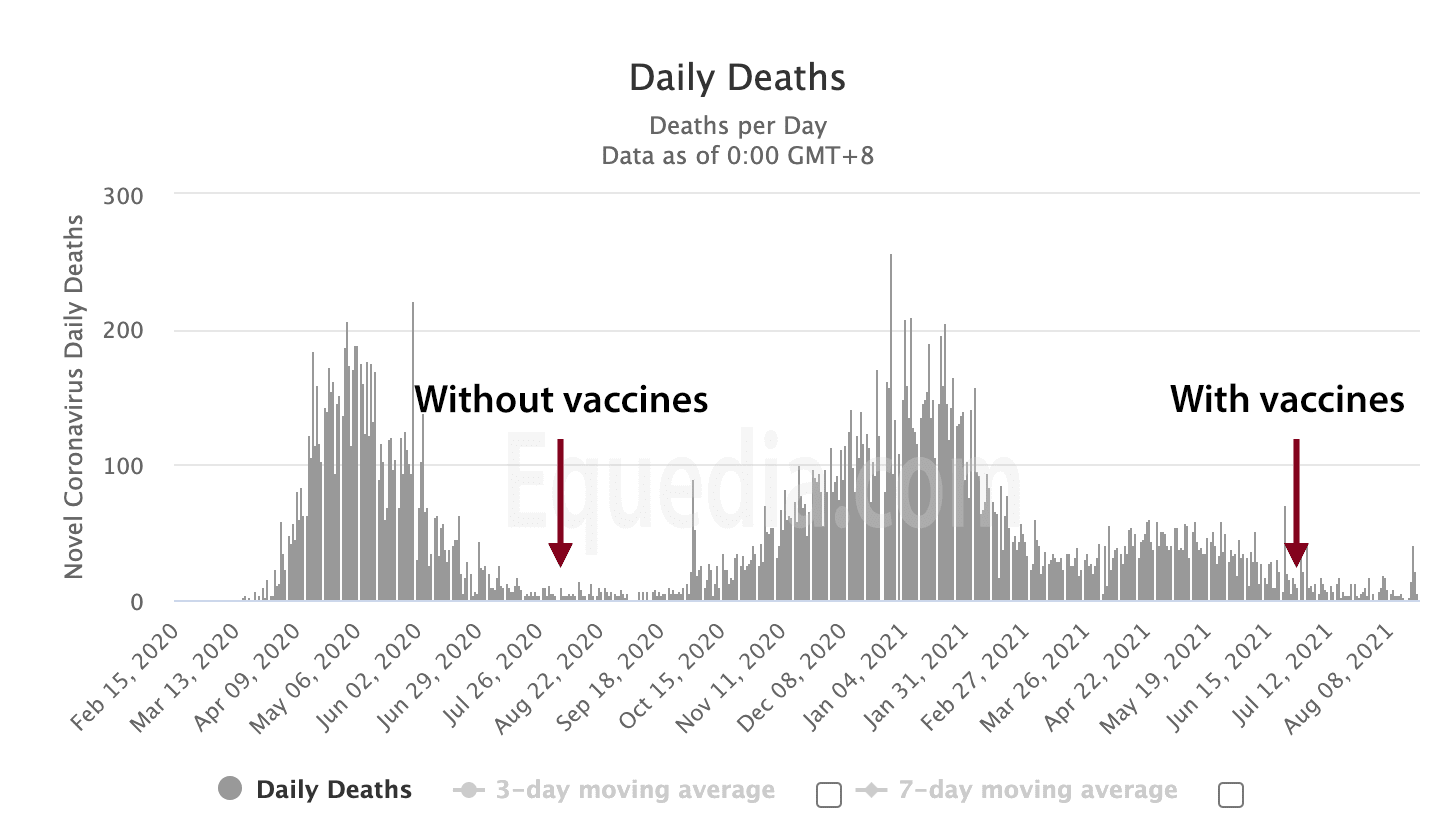
https://www.worldometers.info/coronavirus/country/canada/ – graph-cases-daily
Here’s the most important part.
The media and government have a hard message that everyone needs to be vaccinated because it prevents infection, transmission, and hospitalizations: the mRNA vaccine must be put into everyone to stop this pandemic.
But none of that is accurate when you look at the actual studies that have taken place.
And especially if you look at the science of mRNA and what it is designed to do.
In fact, one could argue that the mRNA vaccines are causing more mutations of the COVID-19 virus.
Transcribed via Fox News, from Canadian viral immunologist and vaccine researcher Dr. Byram Bridle, when asked if the unvaccinated are causing cases to go up:
“Absolutely, it’s untrue to be calling this a pandemic of the unvaccinated. In fact, I would argue, and it’s certainly untrue, this flipping of the messaging (re: Dr. Walkensky) to scare people into thinking that the unvaccinated are somehow driving the emergence of novel variants. This goes against every scientific principle that we understand.
The reality is, the nature of the vaccines that we are using right now and the way we’re rolling them out, are going to be applying the selective pressure to this virus to promote the emergence of new variants. Again, this is based on sound principles.
We have to look no further than chemotherapy for cancers and the emergence of antibiotic-resistant strains of bacteria.
The principles are this: If you have a biological entity that is prone to mutation — and the SARS-CoV-2, like all coronaviruses, is prone to mutation — and you apply a narrowly focused selective pressure that is nonlethal, and you do this over a long period of time, this is the recipe for driving the emergence of novel variants.
And that’s exactly what we’re doing.
Our vaccines (MRNA) are focused on a single protein of the virus, so the virus only has to alter one protein, and the vaccines don’t come close to conferring sterilizing immunity.
People who are vaccinated still get infected; it only seems to be particularly good at blunting the disease, and so what that tells you, therefore, is that these vaccines in the vast majority of people are applying a nonlethal pressure, narrowly focused on one protein, and the vaccine rollout is occurring over a long period of time. That’s the recipe for driving variants.
…if anything, the unvaccinated are likely acquiring natural immunity in pretty substantial numbers, which I would argue from an immunological perspective is going to be much more protective than the vaccine-induced immunity against novel variants.”
Dr. Byram Bridle goes on to discuss the many papers that show that natural immunity is by far superior to any vaccine, especially against novel variants.
One of these studies Bridle referred can be found here: https://www.nature.com/articles/s41577-020-00460-4
The rationale is very simple.
When your immune system fends off a virus, you gain both antibodies and T cells against all parts of that virus, not just the spike protein (as the mRNA vaccines do.) In fact, the mRNA vaccines are so specific to a particular protein that all the virus has to do is mutate and target a different protein.
Perhaps that’s why the Delta Variant is running rampant amongst those vaccinated.
Via National Geographic, August 20th, 2021:
“A preliminary study has shown that in the case of a breakthrough infection, the Delta variant is able to grow in the noses of vaccinated people to the same degree as if they were not vaccinated at all. The virus that grows is just as infectious as that in unvaccinated people, meaning vaccinated people can transmit the virus and infect others.”
So regardless of what a meme on Twitter tells you, every preliminary study I have found shows that the vaccinated can transmit COVID-19, while the Delta variant is just as infectious for both vaccinated and the unvaccinated.
If that remains true, and all signs point to that being the case, then the vaccinated may be the biggest spreaders of the virus – since the mRNA vaccines blunt the symptoms, and the vaccinated might have zero clue that they’re sick.
So what’s the point of taking these mRNA vaccines?
The Delta Variant
According to Dr. Peter McCullough, the Delta variant contains three different mutations, all in the spike protein. This is why it can evade the vaccinated; the vaccinated are protected only against that specific spike protein.
McCullough is a leading medical researcher and one of the most widely published medical scholars in the world in his expertise. In addition, he is an expert in the field of heart and kidney, an editor of two major journals, and an accomplished research scholar.
On June 30th, 2021, McCullough said:
“It is very clear from the U.K. Technical Briefing that was published June 18th that the vaccine provides no protection against the Delta variant. It’s a very mild variant.
Whether you get the vaccine or not, patients will get some very mild symptoms like a cold, and they can be easily managed…Patients who have severe symptoms or at high risk, we can use simple drug combinations at home and get them through the illness. So, there’s no reason now to push vaccinations.”
Here is the U.K. technical Briefing he is speaking of, which shows that the vaccinated are not protected against the Delta variant:
Given the headlines you have seen on the dangers of the Delta variant, why would McCullough say that the Delta variant is a mild variant?
The answer lies in how viruses work.
According to Brian Hooker, Ph.D., P.E., Children’s Health Defense chief scientific officer and professor of biology at Simpson University, the Delta variant is likely more transmissible, but it’s also likely less pathogenic.
Brian Hooker, via Children Health Defense:
“What we’re seeing is virus evolution 101. Viruses like to survive, so killing the host (i.e., the human who is infected) defeats the purpose because killing the host kills the virus, too. For this reason, new variants of viruses that circulate widely through the population tend to become more transmissive but less pathogenic. In other words, they will spread more easily from person to person, but they will cause less damage to the host.”
Hooker said the more the variant deviates from the original sequence used for the vaccine, the less effective the vaccine will be on that variant, which could explain why fully vaccinated people are getting infected with the Delta variant. But this isn’t the case for natural immunity, he explained.
“The vaccine focuses on the spike protein, whereas natural immunity focuses on the entire virus.
Natural immunity — with a more diverse array of antibodies and T-cell receptors — will provide better protection overall as it has more targets in which to attack the virus, whereas vaccine-derived immunity only focuses on one portion of the virus, in this case, the spike protein. Once that portion of the virus has mutated sufficiently, the vaccine no longer is effective.”
Now, there have certainly been times in history that viruses have mutated to become more deadly. In fact, the so-called media fact-checkers quickly pointed this out.
Via Associated Press:
“CLAIM: No virus has ever mutated to become more lethal. As viruses mutate, they become less lethal.
AP ASSESSMENT: False. There are documented cases of viruses becoming more deadly.
THE FACTS: As the spread of coronavirus variants raise new public health questions, social media users are sharing misinformation about how viruses mutate.
A post on Facebook reads, “In the history of virology, there has never, EVER, been a viral mutation that resulted in a virus that was MORE lethal. As viruses mutate, they become more contagious/transmissible and LESS lethal.”
But in fact, there have been cases of viruses that mutated to become more deadly.
“That claim as a whole is just nonsense,” said Troy Day, a professor of mathematics and biology at Queen’s University in Canada, who has studied the ways infectious diseases, including coronavirus, can evolve.
Some examples of viruses that became more deadly over time include those that developed drug resistant variants, and animal viruses such as bird flu, which were harmless to humans initially but then mutated to become capable of killing people, according to Dr. Amesh Adalja, a senior scholar at Johns Hopkins University’s Center for Health Security.
“Flu viruses have developed resistance to certain antivirals that make them more difficult to treat, and therefore make them more deadly,” Adalja said, also noting the same has happened with HIV and certain Hepatitis C strains.”
To be fair, it is absurd to say that there has never been a viral mutation that resulted in a more lethal virus.
But experts never said, “no virus has ever mutated to become more lethal.” A random social media post did. Do you take your investment advice from Twitter memes?
The reality is that, generally, viruses do mutate in hosts and become less lethal and more transmittable. But that’s not always the case – especially in the examples given by the AP fact-checker.
While the AP Fact-check ignorantly highlighted a highly inaccurate Twitter post, it did reveal something troublesome.
“…Some examples of viruses that became more deadly over time include those that developed drug-resistant variants…Flu viruses have developed resistance to certain antivirals that make them more difficult to treat, and therefore make them more deadly…”
Note the words drug-resistant and antivirals – both of which are created in a lab. In other words, the deadlier mutations almost always occur when we’re not using our own immune system to fight the virus.
According to research published last week in Scientific Reports via Nature, the highest risk for establishing a vaccine-resistant virus strain occurs when a large fraction of the population has already been vaccinated, but the transmission is not controlled.
Here is that research: https://www.nature.com/articles/s41598-021-95025-3#Sec2
Given that we know that the Delta variant is just as transmittable amongst the vaccinated, it appears that the transmission, despite the vaccines, isn’t being controlled. And based on the AP Fact-check, this could create a deadlier version of the virus. Furthermore, the virus will continue to mutate and grow amongst our populations because the vaccines don’t actually lead to the death of the virus – that’s why the vaccinated can still transmit and catch COVID-19.
Do you know what does kill COVID-19 with certainty? Ivermectin. In vitro, anyway.
Now, despite all of this, the message that vaccines are necessary continues to run rampant.
So let’s take a look at real-world data.
Are the Vaccinated Superior to the Unvaccinated?
We have already seen from preliminary reports, specifically the U.K. briefing, that the vaccinated are just as likely to transmit the diseases than the unvaccinated.
But let’s expand our scope a bit.
Israel is a world leader in vaccinating its population against COVID-19.
However, earlier this month, Dr. Sharon Alroy-Preis, Israel’s Director of Public Health Services, told us that half of all COVID-19 infections were among the fully vaccinated, and they are seeing signs of more serious disease among them.
Via Bloomberg News:
“Half of the infections in Israel now are among the fully vaccinated, and public health officials are beginning to see signs of more serious disease among them.”
It didn’t take long for Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, to talk about this.
In fact, he said that “95% of the severe patients are vaccinated, while 85-90% of the hospitalizations are in fully vaccinated people.”
Video source here.
This is happening right here in N. America, as well.
A CDC investigation of the July outbreak in Barnstable County, Massachusetts, revealed that 74% of those tested positive for COVID-19 were fully vaccinated.
Furthermore, of the five who were hospitalized, four were fully vaccinated.
Here’s the research: https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w
The CDC also revealed that the fully vaccinated individuals who contract COVID have as high a viral load in their nasal passages as unvaccinated individuals who get infected.
It’s a fact: the vaccinated are just as infectious as the unvaccinated.
Via NBC:
“The internal CDC presentation concluded that “breakthrough infections may be as transmissible as unvaccinated cases.”
This may be shocking at first – especially for those who are fully vaccinated. But, now that you know how the mRNA vaccine works and how the virus mutates, is it still so shocking?
Conclusions
Is COVID-19 real? Absolutely.
Can it be dangerous for a small subset of people? Absolutely.
Have these mRNA vaccines saved lives? Probably.
But given the rapid deployment of mRNA vaccines worldwide, I am most certainly concerned about the long-term effects of this. You should be too.
Do the risks really outweigh the reward, considering that many who catch COVID-19 are asymptomatic or experience very little to mild symptoms? Time will tell.
Will these shots degrade our immune system in the long term? No one knows.
Given how quickly this virus mutates, how many boosters will be required every year – especially since the current vaccines are so specific in their target effectiveness?
Moderna and other mRNA vaccine makers are already testing variations of boosters to attack the Delta variant. Source here.
How many boosters will it take for you to say, “enough is enough?”
In fact, given how the virus mutates and how these vaccines work, we may never achieve herd immunity.
Via The Guardian:
“Reaching herd immunity is “not a possibility” with the current Delta variant, the head of the Oxford Vaccine Group has said.
Giving evidence to M.P.s on Tuesday, Prof Sir Andrew Pollard said the fact that vaccines did not stop the spread of Covid meant reaching the threshold for overall immunity in the population was “mythical.”
“The problem with this virus is [it is] not measles. If 95% of people were vaccinated against measles, the virus cannot transmit in the population,” he told the all-party parliamentary group (APPG) on coronavirus.
“The Delta variant will still infect people who have been vaccinated. And that does mean that anyone who’s still unvaccinated at some point will meet the virus … and we don’t have anything that will [completely] stop that transmission.”
Whether you are for the COVID-19 vaccines or not, this is real information that everyone should have access to.
Fact-check the contents of this letter. Read the actual reports. Ask questions.
Don’t just refer to memes suggesting mRNA vaccines are safe because our other vaccines are safe; those vaccines have had years of long-term studies – the COVID-19 vaccines have zero. The billions poured into mRNA vaccine research helps, but no amount of money can buy time.
You’re not an anti-vaxxer simply because you don’t trust in the COVID-19 vaccines yet, or because you ask questions. Every vaccine is different – especially the mRNA ones. If vaccines were all the same and all it took was money to create one, we’d never be sick again.
And while there remain a plethora of vaccines being tested, I think the next big thing for COVID-19 will be treatments. For example, the U.K. just approved Ronapreve, the first monoclonal antibody treatment for COVID-19.
And there are numerous treatments aggressively being studied, including antivirals such as Ivermectin and Remdesivir.
Perhaps the elites know something we don’t, and that’s why they have been buying up luxury underground bunkers.
Are they preparing for a black swan event, just as tech company Palantir has done by buying gold?
I bet that as the weather gets colder, COVID-19 cases will rise again, leading to more lockdowns – despite the majority of the population having been vaccinated. Even though the data shows that the mRNA vaccines are ineffective against the variants, politicians will implement mandatory vaccine mandates.
This will create volatility, especially for traders. But for investors with a longer-term approach, investing in novel technologies, green tech, infrastructure, energy, and COVID treatment drugs are smart moves.
Do you believe in mandatory vaccines?
Has this information changed your mind at all?
Did politicians use the pandemic to gain power?
Do you think we’re still in a pandemic?
How many boosters will be too many?
Are you worried about the long-term effects of the mRNA vaccines?






Generally, your articles are clear and informative. This one is labored. With that said, the info on Ivermectin was very informative. Also, the aspect of altered protein that is effected.
Ivan, Totally respect all you wrote. Well done – not sure what to think anymore. Its all very exhausting. All we know is that not getting vaccinated puts one socially and with work in a very difficult position. Retaining this stand, while it is not as impossible as holding back a tide (as that is impossible.) It is very very difficult. So I for one am now vaccinated. The drug you mention is it not to counter parasites in animals? Not sure I would be more keen on ingesting that. Anyway food for thought LOL.
Thank you, very informative.
The global vacc-tion effort is part of the bigger plan of global re-set and control over world population under one govt. most people are not aware of what you have so thoroughly described. Keep up the good work.
Excellent report. Thank you for having the courage to write the truth.
There are so many inconsistencies regarding this virus and its worldwide spread, that one could debate for hours on them all.
But the one that I think stands out and is favorable to a very narrow field of view, is the entire ‘suppression of viable, alternate treatments (Ivermectin, Hydroxychloroquine) over the pushing of experimental drugs’. The use of these would get us all to that ‘herd immunity’ so touted by all.
At the core of this, I can see only two possible explanations. The first is a simple ‘follow the money’ scheme that involves all (near) of the elite from the medical fields, the MSM, and political leaders, all conspiring to provide ungodly profits for Big Pharma. It is true that the hierarchy of each of these fields is a very controlling one, and that all subordinates must ‘tow the line’ or face severe disciplinary measures (which we have seen over and over), but this is lacking as a viable reason.
The second involves all of these same people and conditions with the addition of other elitists bodies (WEF, UN, IMF), pursuing an agenda that clearly does not entail the best for mankind. They have openly promoted their depopulation hopes and plans for a ‘reset’ of our civilization. They thrive on chaos and a virus/vaccine-one two punch- would an excellent way to give them both. Given the lies/deceptions, which of these do you think is the true explanation?
Why no investment into testing of antibodies, T cells, antigens of those who recovered naturally producing immunity? I recovered from an 8 day Covid virus fever and have not been reinfected after international homelessness – meaning countless contacts with vulnerable populations.
Informative and, as you pointed out several times, can support either position to one degree or another.
However I believe real world info,at least as seemingly reported by the media, trumps most of these stats
and also your ongoing “heat” thesis.
Fl, CA and to a lesser extent TX all have warmer climates. They all have done worse this summer than last summer-(on per capita hospitalizations and deaths) . FL and TX have also done worse than CA on
vaccinations and much worse on hospitalizations and deaths.
The theory has always been that these places(especially FL) get so hot in summer that everyone
stays indoors more in summer(probably true except for nursing home patients who stay indoors
most all the time and have died far less frequently since vaccinations).
There are other real world points to argue-but I dont understand what the motive is for governments
to press for these vaccines(by the way old FLU vaccines need boosters each year and are rarely
totally effective in the year we get the shots)unless they are the best we have to minimize overall suffering and lockdowns, etc.
I chuckled when Google told me that this email might be “unsafe”
“Do you believe in mandatory vaccines?”
Mandatory vaccines are a violation of the Nuremburg Code
Undisclosed, Graphene Oxide has been found found in the MRNA vaccines. (Fact) Why?
Thanks for spreading the word.
America’s Frontline Doctors is another good source.
H2O2 protocols, H2O2 was used when there was a shortage of N95 masks last year. They were all gathered in trailers and it was used to kill the virus. Then the masks were given back to the hospitals.
Wow, you are so close minded. This article is well researched and on point.
the Nobel Prize winning scientist that invented the PCR test said it was to NOT be used to diagnose, but only for lab use. Funny how he died 3 months prior to the covid outbreak.
You asked where did the virus came from……it has been proven…….Communist China.
Why was Joe and Hunter Biden in China via Air Force-2?? Was Dr. Fauci with them??
Did the Biden’s set up the virus with Communist China to destroy Trump’s economy??
Did the virus get out of control……world wide by mistake?? Why does Hunter Biden get $500K
from Communist China for paintings that look like a 8-year old did??
Why do the Democrats preach Socialism when they really mean Communism??
Democrats are not stupid, they know brainwashing really works, especially on youth.
Obama supported and pushed BLM to invoke mass racism in the U.S.
Democrat Govs and Mayors allowed and supported riots via stand down Police & Fire Dept.
Then they push infrastructure bill so taxpayers pay for their damage, what a joke.
Don’t forget the voter fraud strong in those 5-states. Videos, photos, affidavits of proof and no FBI investigations at all. But Christafer Wray has over a thousand FBI Agents on the Jan. 6 D.C. of taxpaying Americans that wanted justice and got jail time……..can you smell Communism??
How about the Clinton’s hit-men hanging Jeffery Epstein, now that makes over 30 people the
Clinton’s have had murdered during their political careers. Why are they above the law??
Yes, the Communist Democrat Party have a good thing going by BRAINWASHING Americans and
buying the wealthy, notably George Soros (not his real name) a Nazi and Hitler supporter for sure.
We can’t forget the Democrats Communist media…CNN, ABC, NBC, MSNBC, Facebook, Twitter etc.
A lot of puzzle pieces that could be neatly put together but would be washed away by FAKE NEWS.
Dear Ivan,
You did a reasonably good job at describing the current state of affairs regarding covid-19 and the vaccines. But I have also done a lot of research from source documents, including the CDC, JAMA, the FDA, The WHO and the drug manufacturers themselves.
The level of VAERS related deaths to the roll out of the gene therapies, which is what the FDA defines these mRNA based shots as, is 200+ times higher than the level under which all other new medicines etc. that have been released to the public have been previously, throughout history, been suspended. In other words, the monitoring systems go to high alert when the reported deaths approach 25 and are stopped from distribution to the public at 50 deaths. Yet this time, this did not happen. Why not? What is behind the change in policy this time? What makes this situation so special as to allow 200+ times more deaths and counting from the distribution of an experimental medical intervention.
2. The shots are clearly identified by the FDA on their website, as not being vaccines in the previously understood scientific sense since, as the FDA points out in the section of their website where the EUA documentation is reviewed and disclosed, there is no biological genetic material in those shots from the SARSCOV-2 itself. Therefore they are only called vaccines to give legal cover to the pharmaceutical companies that are manufacturing these shots under US Government sponsorship. You will also discover that the mRNA technology and creation was entirely funded by various US Government Agencies over the previous 30 years.
3. The EUA applications on the FDA website, to gain permission to distribute the gene therapies included clinical trial data on the efficacy of the vaccines in assisting covid infected patients in the recovery from the virus. The control group was given a placebo. This data, submitted with the applications was dissected by Dr. Fleming in a 4-hour video analysis ( links available upon request) where the data submitted by the drug makers themselves showed only a 1% difference in recovery rates from covid, versus the control group on all markers, including deaths, and adverse reactions. This basically non-existent efficacy improvement of 1% in favour of the vaccines is for a virus with a known recovery rate, based on now available data, of about 99.8% for those who have had the virus and received no medical treatment.
4. The US Government has a website that clearly states the current shots are part of a “clinical trial” that now runs until May 2023 or so. The current shots have not been proven safe by the FDA or any other health authority. All claims by Health Canada, Justin Trudeau etc. that say the “vaccines” are safe are blatant lies and misdirection – and deliberate ones at that.
5. My body, my choice! This applies to whether I decide to take the vaccine or not. This choice is protected by the Nuremberg Code of which Canada is a signatory. This right is being ignored and steamrolled over by any number of Governments in Canada and elsewhere. Why?
6. Doctors can only prescribe and deliver the shots once they have given their patient information for that patient to have “informed consent” – a legal as well as a moral and ethical obligation per the Hippocratic Oath etc. This is not happening and all such shots are “crimes against humanity” as defined under the Nuremberg code. How can this be proven? Well, for one thing, the vaccine inserts themselves upon which Doctors may normally use to educate themselves on any known or possible adverse reactions are blank. If I ask to see said inserts they are blank, the one from Moderna makes a note on the multi-page insert that “They are intentionally blank”.
7. The Ontario and other Governments have repeatedly lied about covid death counts and have cooked the books to favour a higher death total than is otherwise the case. This is like a business having two sets of accounting books. The Ontario Ministry of Health admitted on its website in August 2020 for example, I have the printouts from those pages, that since the covid death stats were low, compared to those of other authorities in the US and European jurisdictions, they arbitrarily boosted the numbers by 50% to bring them in line with international stats. They are any number of sources showing how Doctors have been pressured into putting down covid as the cause of death. Mr. Floyd who died in Minnesota, yes I have watched the videos several times. has covid listed on his death certificate (died with covid) – he clearly died from a drug overdose as per the autopsy, so why the covid reference? I know the answer to that question.
7. The PCR test, you do an okay job of reviewing it. But here is a fact check for you to do: go to the original patent filed by the inventor of the PCR test Kerry Mullis (I believe he won a Nobel Prize for his efforts). Read the document and you will note that he recommends in the patent that no more than 20 cycles be run and that any cycles above that level will generate statistical noise. Yet Fauci, recommends 30 cycles and various other Health Authorities use 35 or higher and Ontario has changed their cycles with at times recommending 40 cycles. At 50 or more cycles, according to some experts (unverified or fact checked by me, just what I read) 100% of people would be diagnosed with covid – mostly asymptomatic.
You will note the change in narrative from Ontario around June\July 2020 when the daily announcements moved from covid death (not enough of them) to case counts and how the case counts kept rising during the summer, when flu viruses traditionally, are not a health risk. Why?
You can surmise from this, that you can dial up or down the case count like changing the thermostat on your furnace, more cases needed just up the cycles used, less cases wanted, lower the cycle count. And of course, the more people tested and the higher the case count, the lower the incidence of covid infections in the population. Funny that eh?
8. You clearly, and likely unknowingly, subscribe to the Germ Theory of human health and disease. The Germ Theory basically says that all pathogens that are bad for human health come from outside the body and thus can be and must be defended against. This theory was first endorsed and promoted by, any surprise, the US Army College of War! So be afraid of invisible invaders you cannot see nor defend against and do not trust your own body’s immune response (their really is no “immune system”) per se.
9. You fail to explore the Terrain theory of health, and seem to be unaware of the philosophical battle between Pasteur and Beauchamp. Pasteur on his death bed reportedly (unconfirmed by me) stated that the Terrain Theory is valid and the better way of understanding human health and disease. And if you did deeper and really did your homework, you will find that most disease outbreaks coincide with the introduction of new electronic technology, or other toxins that invade and poison the human body. This includes DDT which was tied to Polio – DDT summer spraying stopped in North America, and Polio was eradicated.
10. You fail to review known adjuvants in the shots that are harmful to human health and promoted as safe on the Health Canada website such as SM-102 – a known toxin. Another know toxin, which comprises the majority of the liquid in the covid vials, as confirmed by a Spanish academic group, and yet to be independently verified, is graphene oxide, again another known toxin to human health. Lots of info on this also.
11. An Alberta Court heard from the Chief Medical Officer of Health, Deena Henshaw herself, on July 21st, during a court case on covid mandates – mask wearing, social distancing, lock downs etc., that the Province or Ministry of Health was unable to provide any evidence or documentation, such as White Papers upon which the Province based its Emergency Measures, to the Court as requested by the Defendant, under a subpoena. While Mr. King lost on a procedural point on his objection to the $1,200 mask violation infraction, he is jubilant that he has scored a victory in the “court of public opinion” through the admission, on the Court Record, that no evidence is available to support the allegation that covid-19 exists in a biological form in nature.
12. I can keeping going, but I need to get some sleep. So one last point. In late March 2020, the WHO, on its website officially downgraded covid-19 “from a highly infectious disease” to the same level as the seasonal flu. The British Government also published a similar official finding on one of their websites. That did not stop the Brits from bringing in their Emergency measures legislation and lock down mandates the next day…..So the Pandemic ended in March of 2020 but no one seems to know that. Just like Ontario revoked its Emergency legislation around covid on June 9th, likely in response to the constitutional challenge by noted lawyer Rocco Galati. in late May. Hard to go to Court to fight a law that no longer exists. Only to be replaced by the Ontario Re-Opening legislation – which I have not read as yet.
I am in the investment business and like reading your thoughtful comments and research, although I do not use it for any investment purchases. You were brought to my attention by a client. I am more concerned about the medical tyranny that covid represents than how to make money from it. I refuse to invest in tech that will be used to enslave me. What use is money if I have no liberty? For example, without a vaccine, I am unable to travel to my new, personally owned, Waikiki timeshare unit. Bought 5 days before Trudeau imposed travel restrictions and lockdowns.
But I believe there is more to life than just money. What about you Ivan?
You can call me on my cell at any time. Email me and I will give you the number as I do not want it published. Jack.
Thanks for putting all this together. Would be interesting to see what happened to Novavax . This is a classic vaccine with (seems to be) higher effectiveness. Trudeau said the newly renovated facility in Montreal will buy some manufacturing capacity and then he seemed to change it for Moderna. All very shady deals that may bring light to the question why mRNA only.
Thanks
Congratulations on an amazing piece of research.
(and Ivan of course).
I am very confused as most people are but what scares me the most is the suppression of information.
http://www.ads4truth.org/, dr jane orient and so many others who apparently were very respected medical authorities until they disagreed with big pharma and government.
I THOUGHT THIS WAS AN INVESTMENT PAGE
Great article Ivan , on the issue of mandatory jabs , it must be NO , personal freedom is not totally dead is it ?? The poloticians around the world [ and the hidden bodies , that really run the world ] have definately used this Covid pandemic to tighten their grip on everything [ cash was being percieved as a major way to spread the disease , but no mention of non contactless cards and readers ] they will use this to eliminate cash within a decade , therefore reducing the so called middle classes down another level , yet again . The great wealth divide will get worse and trouble will eventually break out in many city’s throughout the world . I am very sceptical of the whole political system On a personal level , my daughter was one of those in the UK , left paralyzed by the AstraZeneca drug and it was no surprise , that I did not recieve an answer to my email requesting greater help for those affected , from the CEO of Astrazeneca
Ivan this is the 1st time in the many years I’ve been reading your articles that I’ve truly felt compelled to connect. I encourage you to continue the research and to push it out as far and wide as possible. I will do my part and share it with my circle.
To Jack DiNardo:
I couldn’t find evidence to your #12. In fact on WHO’s homepage one of the FAQs states:
Q.: “When will this pandemic end so things can go back to normal?”
A: “We don’t know when the pandemic will end, but we know it depends on every person’s contribution in helping stop the spread of the virus. …”
To your #10 (grahene oxide”): You can’t idenify Graphene Oxide via microscope as the Spanish group did. That this labile compund comprises the majority of the liquid in the vaccine isphysically and chemically not possible.
Your #7 (the second #7, number of cycles) may have theoretically a valid point.
Alfred
I have had Covid-19; almost-certainly Delta, since I got infected in early August. I know exactly who the index case was too (that is, how I got it and from whom.)
I was not vaccinated, on purpose. I hit it immediately with meds and am fine. It was rough and definitely not fun, BUT I now have extremely robust natural immunity and, from recent return to my regular exercise regime, the metabolic damage was *LESS* than the viral infection I got in January 2020, which was almost-certainly H1N1 influenza.
Will I EVER take a jab at this point? No. Under no circumstances, because there is no reason to. You’d never take a measles shot IF YOU HAD THE MEASLES, despite the MMR shot being very (100x to 1000x or more) safe compared against the Covid-19 shots. Why? Because you can’t benefit from it; you already had the measles. There is NEVER a medical argument for a drug or treatment where no benefit is available since there is NO SUCH THING as a treatment or drug without risk. If the benefit is zero then there is NEVER a reason to accept such.
We all need to make an individual choice. Packing on an extra 100lbs is a choice and, in the context of Covid, makes a bad outcome a LOT more likely. Well?
I’m 58. I had Delta Covid-19. I recovered. I’m now sterile immune and will walk into a Covid-19 ICU unit with no PPE and zero fear. If you took the shot instead, and have not had the infection, are you equally willing to do so right next to me?
If not what does that say about your faith in your decision?
Just asking, you know….
No. i don’t believe in mandatory vaccines.
The roll out of Gardasil vaccine is a good example, my daughter suffers from brain stem effects from taking this. Look at all the more severe cases including deaths within days. All rolled out in the public schools to our youth – who are still developing, & aluminum as a transfer agent in the first doses. Aluminum is a poison to our body & some individuals cannot tolerate it. There was never any research or anything presented to parents on this vaccine & its development, just how great it is & its good for prevention !!! LOL.
there have been facebook groups & such on this vaccine but all have been deleted, they don’t want you talking about the negative.
Dear EQUEDIA people,
thank you so much for your research, for this very enlightening letter. My friend worked for more than 30 jears in hospital and she refused from the beginning to be vaccinated. I’m happy I didn’t interfere.
Being an engineer the statistics were persuasive: so I’m vaccinated.
With kind regards
Robert from Berlin
Excellent analysis! Thank you. At best, it shows a completely incompetent, negligent and cruel over-reaction by governments, health authorities and so-called ‘doctors’ to an influenza outbreak. At worst it reveals a global conspiracy by sick, psycopathic authoritarians to use a flu epidemic to impose Marxist tyranny, destroy society, kill people and implement UNAgenda2030. It appears that the entire Covid scam is merely an excuse to inject people with genetic altering material for either profit or population control…or both. One would like to believe that somewhere there are leaders with enough integrity, intelligence and humanity to put an end to this madness. Unfortunately they don’t appear to exist.
You make a good case for staying unvaccinated now that vaccinated numbers are showing their true colors. However, the initial problem was that COVID-19 cases, deaths & hospital visits were spiking rapidly & something had to be done about it with or without a vast amount of data/science/studies to rely on. After mRNA vaccines were administered, all these dramatically fell, & even today you may get sick (w/ delta) and or spread the virus, but death & hospital visits for many are a thing of the past. With at least some COVID-19 containment, drug manufacturers can focus, test, study etc. long-term implications, target effectiveness, other variants & mutations, & determine what other products or course of actions can be used to ‘put the fire permanently out’ so do speak. Yes, the jury is still out on whether or not it was worth being vaccinated, but based on what we’re seeing in the populous today, I wouldn’t bet against it or the medical profession. I suspect this virus becomes just another annual booster shot at your doctor’s office & am not too worried about long-term effects yet. Politicians like Trudeau are taking advantage of it for a re-election bid but suspect another minority gov’t is in the cards. I do not think the gov’t will make it mandatory but market forces (employers etc.) will force the issue on employees or lay you off. I don’t think were still in a pandemic, just maintenance mode. The power at be are still in control mode & loving it. Excellent work/article. It does raise a lot of questions, but the long and short of it, we will not have any choice sooner or later.
I believe that you have provided a fairly balanced analysis and assessment of the virus. Certainly one of the best I have read. I know that you personally do not agree that the virus is as severe as some present it, from your past writings. Your bias appears to have limited your investigation into statistics that support your bias and increases investigation for stats that favor the vaccine. You know what they say, there are lies, damn lies, and statistics.
An example of this is the reporting of infection rates since the vaccines are available. Your DD needs to correct timeframe to what you say represents when vaccinated people are exposed to the virus. Then we could see what the impact really is. And in Israel, you tout that half of the infected are vaccinated. But, what is the infection raye now versus before the vaccine came out? If the total infections now vs then have dropped say 80%, I would say the vaccine is effective. Also, since the population is predominately vaccinated (say 4-1), the fact that the ratio is not reflected in the infection today shows that the vaccine is effective. The current infections should also be 4-1 for vaccinated vs unvaccinated.
I agree with the questionable testing that has increased the rate of infection. I think that is why they don’t recognize beating the infection gives you immunity. But that is rabbit hole in terms of the impact of the virus. We have high death rates in seniors, and infections in healthy under 50 people that are dying. And healthy people have have ongoing debilitating symptoms that continue to impact them. You may be correct that we don’t know what mRNA might do to us in the future, but it is highly likely it won’t be as bad as what COVID can give you today.
Your statements about the specific protein targeted by the vaccine neglects to identify that the exact protein that makes the virus so virulent, is the one that is targeted – the spike protein. Anything is possible, but a significant change in the spike is more likely to reduce it’s virulence. The vaccine was initially started to target the spike of the original SARS from a few years ago and it turns out they are the same. This is why the the vaccine could be developed so quickly, they had a head start.
I think you did a good job in trying to provoke more thought on the whole COVID situation, but your bias in this report will only serve to perpetuate the fear and poor logic of those with the same bias.
Respectfully,
Ted
The local reports from county health physicians all report that the majority of hospitalized patients are unvaccinated patients at about 85% whereas the majority of population in this area has been vaccinated over 60%. That math suggest that vaccinations are currently very beneficial in preventing serious illness and hospitalization. I have to go by what our local health authorities report as they do not have any agendas.
If you research who is behind these injections you will find it was all planned i would not trust any figures they are a waste of time you will soon find out what is going on.The sheeple have been fooled.
I didn’t do any research on the vaccine. I had the actual virus in 2020. How do I know, I essentially lost all sense of smell and taste for nearly 6 months. It took me literally, almost a month to even notice I didn’t smell that well anymore. I got the vaccine because the company I work for provide a $250.00 bonus to anyone that got it. Otherwise, I would have avoided it like the plague! No serious testing, come on, we’re one big test going on right now!
The media and government have been conducting one giant social experiment with this virus. If your only source of information is the new, then you’re part of the problem, not part of the solution. Several studies that have not be publicized show that those that get admitted to the ICU are vitamin D deficient. A study from Spain shows that once admitted to ICU, administration of vitamin D significantly reduces the severity of the disease. Sure drugs from the pharmaceutical companies may also help, but you can’t patent vitamin D. Follow the money and you are more likely to find truth!
THANKS
i too have heard info from research nurses who are with top tier research facilities who have said vitamin D is the biggest differential to those who live !
i have started a vitamin d regime in the late fall tru mid spring
i also wear a mask in crowds and stores
no ! I depended on Dr’s & nurses I know& the available sight to get vacine
As a retired primary care/ER physician,I have been shocked by the ineptitude and incompetence by virtually all the alphabet agencies and especially western health authorities.
The data of deaths per million in the US and European countries in 2020 fails to provide even a hint of any effectiveness of “lockdowns” : Sweden(no lockdown) vs other European countries and N.Dakota vs S.Dakota,yet the house arrest continued in many regions in 2021.
https://fee.org/articles/lockdowns-not-linked-with-lower-covid-death-rates-new-study-finds/
Yet this,sadly,is only one facet of the Trainwreck.A far more sinister aspect has been the systematic suppression by media and,I am sad to say,government health authorities.
Early in the pandemic,astute front line physicians found a variety of vitamins(like vitamin D) and supplements that had beneficial effects.Throughout 2020 a large amount of evidence accumulated around effective early outpatient treatment by certain repurposed drugs that dramatically reduced hositalizations and deaths:https://covid19criticalcare.com/
Yet,the official advice for patients with mild/moderate respiratory symptoms presenting to or phoning health facilities continued to be:”go home and isolate and take tylenol and come to hospital if breathing becomes difficult”
The “vaccine” was presented as the holy grail and the public gaslighted about the existence of alternative treatment.
Unfortunately,the “vaccine” is now beginning to fail ,as demonstrated in Israel ,one of the most highly vaccinated countries where the majority of hospitalizations are among the “fully vaccinated”.
And in the UK,vaccinated deaths exceed unvaccinated deaths.https://www.visiontimes.com/2021/07/04/deaths-hospital-vaccinated-uk.html
What could explain the curious denial of early outpatient treatment to western countries’ populations over the past ~18 months? I don’t think one needs a PhD to figure this one out!
Totally enjoyed the article as I do the previous ones. People are followers and lazy and therefore do not do their own research. What really irks me is the fact that we have not seen any debates whatsoever from virologistes, immunologists, etc with opposing views. Why is that? If we are supposed to live in a society with freedom of speech why are those opposing doctors/researchers opinions being obliterated? Something doesn’t smell right. Not sure what the agenda is. Maybe buying vaccine producing stocks should be considered. Keep up the great articles and the super research.
Hello everyone,
From experience working in a hospital in Miami, FL I can attest that most of the Covid19 patients requiring hospitalization are unvaccinated. We have also seen fully vaccinated individuals in crisis.
With that being said, I strongly believe that the CDC, Fauci, and the government have done an amazing job at misinforming our citizens and that is in part why the numbers of Covid19 cases continue to grow. People were quick to dish their masks once fully vaccinated.
Vaccines will not keep anyone from contracting and spreading the virus. Therefore, I encourage people to continue to wear their masks and avoid crowded places.
Ivan, as always an amazing job bringing unbiased information to your readers/investors.
Would love to see coverage on Aviptadil/Zyesami. One of the many drugs undergoing trials. I think is extremely effective against Covid19 but what’s hurting it is the fact that it is not a big pharmaceutical company.
Thank you once again!
Trial results you show are Phase 2 and are perfectly legitimate for the grouping of 43000 participants. When you expand this to the Billions of people world wide, 170 cases, or about .004% if the trial participants, translates to 28,000,000 possible unvaccinated cases in the world. Lots of death possible.
You could report the fact that vaccinated people DIE less, and the hospitals are filled with the unvaccinated. And since you are always right minded & money focused, the cost of hospitalizing and burying them is at least as important as the restaurants the shutdowns have caused. Remember at the time of big shutdowns no one knew if this virus could kill most of us. Now we know that vaccines and masks can shut this virus down, but we politicized the solution and fight science in favor of money.
It literally says Phase 3 trial – not Phase 2 – check your facts. You are also completely wrong – its a 170 cases of COVID – almost all of which were little-to-mild symptoms. What in the world are you reading?
If you want to talk about the deaths – there were 15 deaths with COVID WITH the vaccine – and only 14 in placebo group. So if you want to shrink the subset of data, those on vaccines, regardless of why they died, die more. This is the problem – you’re can’t even differentiate between Phase 2 and Phase 3 – even if PHASE 3 is blasted in your face!
To your point: vaccines and masks can shut this virus down. Now, after 9 months, we now know the vaccines not only lose their efficacy (could simply be now we have an expanded data set of more than 170 people), but over a dozen studies show masks don’t work. Full blown clinical studies.
“PFIZER AND BIONTECH CONCLUDE PHASE 3 STUDY OF COVID-19 VACCINE CANDIDATE, MEETING ALL PRIMARY EFFICACY ENDPOINTS”
NOT PHASE 2.
The most significant point made in this report is my hobby horse, the presentation of the statistics. This is the most misleading area of leverage for those in power and are using these numbers for leverage. What is required is a universal system that is similar to the stock exchange indicators of deaths over the last day, week, month, hospital bed occupancy with levels of severity that can be QED. A candle system would be ideal to identify the peaks and average.
There is a very strong point made for alternative treatments, Ivermectin as an example. Where I currently reside these are available and have been found to be extremely effective. This somehow needs to be chased and become the normal like aspirin is, this will go a long way to save lives, screw the money.
Thank you for telling the truth.